The Infection Prevention and Control Committee is concerned about an outbreak of Serratia marcescens in the intensive care unit. If an environmental source is suspected, the BEST method to validate this suspicion is to
When preparing an educational session, objectives should be written using clear, precise language to describe what the learner is expected to learn. All of the following are examples of appropriate objective verbs EXCEPT:
Following an outbreak of Hepatitis A, the water supply is sampled. A high count of which of the following isolates would indicate that the water was a potential source?
The Environmental Services department is purchasing a new disinfectant that is an approved hospital disinfectant with no tuberculocidal claim. This product is appropriate for cleaning which of the following items?
Which of the following factors increases a patient’s risk of developing ventilator-associated pneumonia (VAP)?
Which of the following BEST describes the content of an interpretive surveillance report?
An infection preventionist (IP) is asked to evaluate a series of published sources about CAUTI prevention strategies. Which source shows the strongest evidence for the IP to implement change?
A surgeon approaches an infection preventionist (IP) concerned that there are more surgical site infections (SSIs) in hysterectomies performed in the facility's stand-alone surgery center than in those performed in the acute-care operating room. The IP should
In order to ensure accurate calculation of central line days, which of the following is TRUE?
Which of the following intravenous solutions will MOST likely promote the growth of microorganisms?
Which of the following options describes a best practice for avoiding occupational health hazards in a healthcare facility?
Which of the following patients with human immunodeficiency virus infection requires Airborne precautions?
Two patients in a medical intensive care unit (ICU) and one patient in a surgical ICU have Aspergillus fumigatus cultured from sputum. An exterior construction project was started two weeks ago with demolition of an old office building one week ago. All of the following questions are important for the infection preventionist to ask EXCEPT:
The expectation to call out or speak up when an infection prevention lapse is observed is an example of
The rate of catheter-associated urinary tract infections (CAUTIs) has decreased following recent practice changes. To present these results to the Quality Committee, the infection preventionist should use:
Which of the following pathogens is associated with the highest risk of seroconversion after percutaneous exposure?
During the past week, three out of four blood cultures from a febrile neonate in an intensive care unit grew coagulase-negative staphylococci. This MOST likely indicates:
Healthcare workers are MOST likely to benefit from infection prevention education if the Infection Preventionist (IP)
In the Preparedness and Response Framework for Influenza Pandemics, intervals are used to describe an influenza pandemic progression. The interval “Deceleration of the Pandemic Wave” is characterized by:
An infection preventionist (IP) reviews research from a current publication and compares the data to the IP’s facility data. This is an example of:
Which of the following operating suite design features is LEAST important for the prevention of infection?
A nurse exposed to pertussis develops a mild cough 14 days later. What is the recommended action?
On January 31, the nursing staff of a long-term care facility reports that five out of 35 residents have developed high fever, nasal discharge, and a dry cough. The BEST diagnostic tool to determine the causative agent is:
After reviewing quarterly surveillance data, the infection preventionist (IP) identifies an upward trend in needlestick injuries occurring during bedside blood draws. What is the MOST appropriate collaborative action for the IP to take with the Occupational Health Department?
The Infection Control Department is notified of possible contamination of one lot of dressings. Which of the following actions should be taken?
When evaluating environmental cleaning and disinfectant products as a part of the product evaluation committee, which of the following is responsible for providing information regarding clinical trials?
Which of the following is included in an effective respiratory hygiene program in healthcare facilities?
Which of the following anti-infective materials is used on endotracheal tubes, urine catheters, and intravascular catheters?
An infection preventionist is informed that there is a possible cluster of streptococcal meningitis in the neonatal intensive care unit. Which of the following streptococcal serogroops is MOST commonly associated with meningitis in neonates beyond one week of age?
What data should be collected and analyzed as part of a syndromic surveillance program?
An infection preventionist reviewing patient records in an outpatient hemodialysis center notes an increase in localized infections at catheter access sites. Which of the following strategies reduces the risk of infection in this population?
Which of the following strategies is MOST effective in reducing surgical site infections (SSI) in orthopedic procedures?
The infection preventionist (IP) is assisting pharmacists in investigating medication contamination at the hospital’s compounding pharmacy. As part of the medication recall process, the IP should:
Which statistical test is MOST appropriate for comparing infection rates before and after an intervention?
A 17-year-old presents to the Emergency Department with fever, stiff neck, and vomiting. A lumbar puncture is done. The Gram stain shows Gram negative diplocooci. Presumptive identification of the organism is
An 84-year-old male with a gangrenous foot is admitted to the hospital from an extended-care facility (ECF). The ECF is notified that the wound grew Enterococcus faecium with the following antibiotic sensitivity results:
ampicillin – R
vancomycin – R
penicillin – R
linezolid – S
This is the fourth Enterococcus species cultured from residents within the same ECF wing in the past month. The other cultures were from two urine specimens and a draining wound. The Infection Preventionist (IP) should immediately:
A 15-year-old is diagnosed with invasive meningococcal disease. Which of the following should receive chemoprophylaxis?
Which of the following BEST demonstrates the effectiveness of a program targeted at reducing central-line associated bloodstream infections (CLABSIs) in an intensive care unit (ICU)?
A patient with shortness of breath and a history of a tuberculin skin test (TST) of 15 mm induration was admitted to a semi-private room. The infection preventionist's FIRST action should be to
Bioterrorism agents are classified according to priority. Which organism is listed as a Category A agent?
How can infection preventionists BEST educate on a new infection prevention protocol for adoption across different departments within an organization?
During a COVID outbreak with hospital-associated transmission cases, the infection preventionist (IP) receives a news media call about what is being done to reduce the transmission. The IP's BEST response is to
A nutrition support team wants to determine whether patients who receive total parenteral nutrition (TPN) at home are at increased risk of central line–associated bloodstream infection (CLABSI) compared with patients who receive TPN in the hospital. The BEST way to compare these two groups is to calculate the:
During the last week in June, an emergency department log reveals numerous cases of profuse watery diarrhea in individuals 74 years of age and older. During the same time period, four immunocompromised patients were admitted with possible Cryptosporidium. Which of the following actions should the infection preventionist take FIKST?
An infection preventionist (IP) encounters a surgeon at the nurse’s station who loudly disagrees with the IP’s surgical site infection findings. The IP’s BEST response is to:
An infection preventionist (IP) is asked to participate on a team to decrease ventilator-associated pneumonia (VAP) rates in a 20-bed ICU. The IP provides the following information. What is the first quarter ventilator utilization ratio?
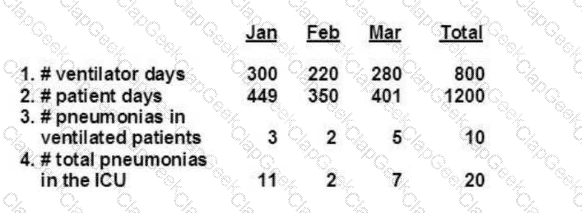
Data Provided (First Quarter):
Ventilator days (Jan–Mar total): 800
Patient days (Jan–Mar total): 1200
An infection preventionist (IP) receives a phone call from a local health department alerting the hospital of the occurrence of a sewer main break. Contamination of the city water supply is a possibility. Which of the following actions should the IP perform FIRST?
When conducting a literature search which of the following study designs may provide the best evidence of a direct causal relationship between the experimental factor and the outcome?
Which of the following is an essential element of practice when sending biohazardous samples from one location to another?
The infection preventionist (IP) is working with the Product Evaluation Committee to select a sporicidal disinfectant for Clostridioides difficile. An effective disinfectant for the IP to recommend is
An infection preventionist is assisting the Product Evaluation Committee in selecting a disinfectant for use in a healthcare facility. Which of the following criteria is MOST important?
What should an infection preventionist prioritize when designing education programs?
The MOST important characteristic to include when using a template for a comprehensive annual risk assessment is
What is the correct order of steps for reprocessing critical medical equipment?
Which of the following statements is true about the microbial activity of chlorhexidine soap?
A patient with fever, rash, and meningoencephalitis is admitted to the hospital, placed in Droplet Precautions, and started on antibiotic therapy. Bacterial cultures of the blood and spinal fluid are negative, and infection with West Nile virus is strongly suspected by the infectious disease consultant. Appropriate control measures should include:
One of the elements of antibiotic stewardship is controlling antibiotic use. Which of the following BEST describes a closed formulary?
A new hospital disinfectant with a 3-minute contact time has been purchased by Environmental Services. The disinfectant will be rolled out across the patient care 3-minute contact time has been purchased by Environmental Services. The disinfectant will be rolled out across the patient care areas. They are concerned about the high cost of the disinfectant. What advice can the infection preventionist provide?
An infection preventionist (IP) observes an increase in primary bloodstream infections in patients admitted through the Emergency Department. Poor technique is suspected when peripheral intravenous (IV) catheters are inserted. The IP should FIRST stratify infections by:
What inflammatory reaction may occur in the eye after cataract surgery due to a breach in disinfection and sterilization of intraocular surgical instruments?
As part of their antimicrobial stewardship initiative, Hospital A is using a qualitative study to assess their program. What type of data will be collected using this approach?
A facility performs active surveillance cultures for methicillin-resistant Staphylococcus aureus (MRSA) on all patients upon admission and weekly. Twenty-two of the patients with positive cultures for MRSA were transferred from outlying facilities. The following MRSA data for a 3-month period are shown. Review of the data reveals which of the following is increasing?

An infection preventionist is developing training exercises for emergency preparedness and disaster response teams. The MOST effective instructional method for retaining information is:
The infection preventionist understands that the heating, ventilation and air conditioning (HVAC) systems in the facility can be a risk factor for healthcare-acquired infections. What is the MOST likely risk from the HVAC system for patients in a Pediatric Oncology unit?
After defining and identifying cases in a possible cluster of infections, an infection preventionist should NEXT establish:
A change in the disinfection protocol is indicated for which of the following scenarios?
Which of the following blood-drawing methods is considered to be a needle-safe practice?
Based on the Spaulding classification, which of the following pairings is an example of a semi-critical item and its minimal level of disinfection?
At a facility with 10.000 employees. 5,000 are at risk for bloodbome pathogen exposure. Over the past five years, 100 of the 250 needlestick injuries involved exposure to bloodborne pathogens, and 2% of exposed employees seroconverted. How many employees became infected?
A healthcare personnel has an acute group A streptococcal throat infection. What is the earliest recommended time that this person may return to work after receiving appropriate antibiotic therapy?
An infection preventionist observing the technologist in sterile processing load the washer-disinfector or washer-decontaminator should expect to see them:
An immunocompetent patient is diagnosed with active tuberculosis (TB). Which of the following sites of the disease is MOST likely to result in transmission to healthcare personnel?
In the current year, cases of tuberculosis (TB) among foreign-born persons accounted for the majority of new TB cases in the United States. The number of states with greater than 50% of cases among foreign-born persons increased from four cases ten years ago to 22 cases in the current year. This information can BEST be used to
heighten awareness among Emergency Department staff.
inform staff who are foreign-born.
educate patients and visitors.
review the TB exposure control plan.
A hospital is experiencing an increase in vancomycin-resistant Enterococcus (VRE) infections in the hematology-oncology unit. Which of the following interventions is MOST effective in halting the spread of VRE in this high-risk setting?
Though basic principles of emergency management remain the same for all types of disasters, which of the following interventions varies to address the specific needs of the situation?
The infection preventionist recognizes that construction barriers are a key component of the Infection Control Risk Assessment (ICRA). The MOST important factor to consider is that construction barriers should:
Hand hygiene rates in the facility have been decreasing over time. The Infection Preventionist (IP) surveys staff and finds that hand dryness is the major reason for non-compliance. What step should the IP take?
A hospital is experiencing an increase in multidrug-resistant Acinetobacter baumannii infections in the intensive care unit (ICU). The infection preventionist's FIRST action should be to:




TESTED 06 Jul 2026
